RINVOQ (upadacitinib) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to methotrexate (MTX). RINVOQ may be used as monotherapy or in combination with MTX or other nonbiologic disease-modifying antirheumatic drugs (DMARDs).


[Affiliates to insert drivers to local asset]
RINVOQ SELECT-COMPARE clinical trial results
Hear Dr. Roy Fleischmann discuss study results in patients with moderate to severe active RA with an inadequate response to methotrexate.1-3


SELECT-COMPARE: Study design
A Phase 3 study investigating the efficacy and safety of RINVOQ + MTX compared with placebo + MTX and adalimumab + MTX for the treatment of moderate to severe RA in patients who had an inadequate response to MTX2
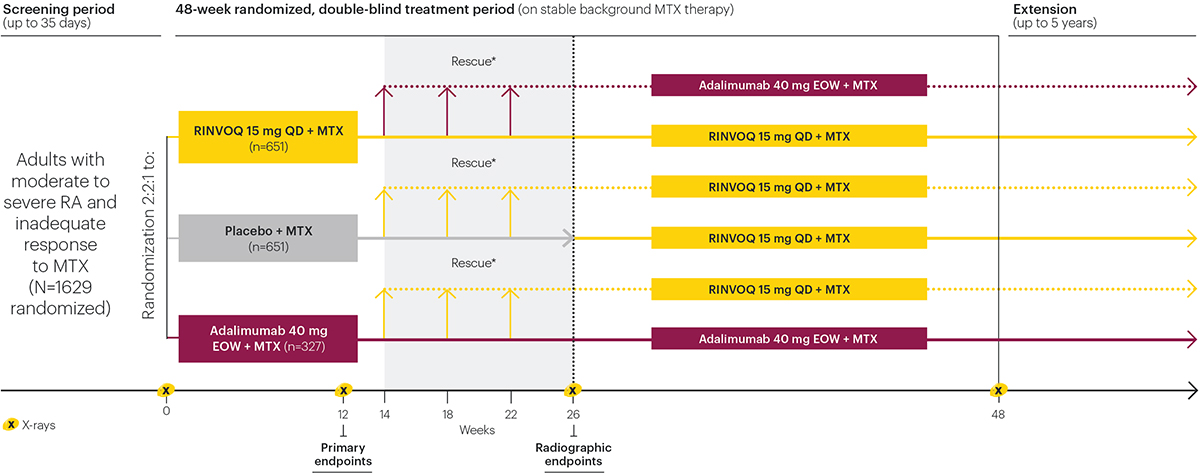
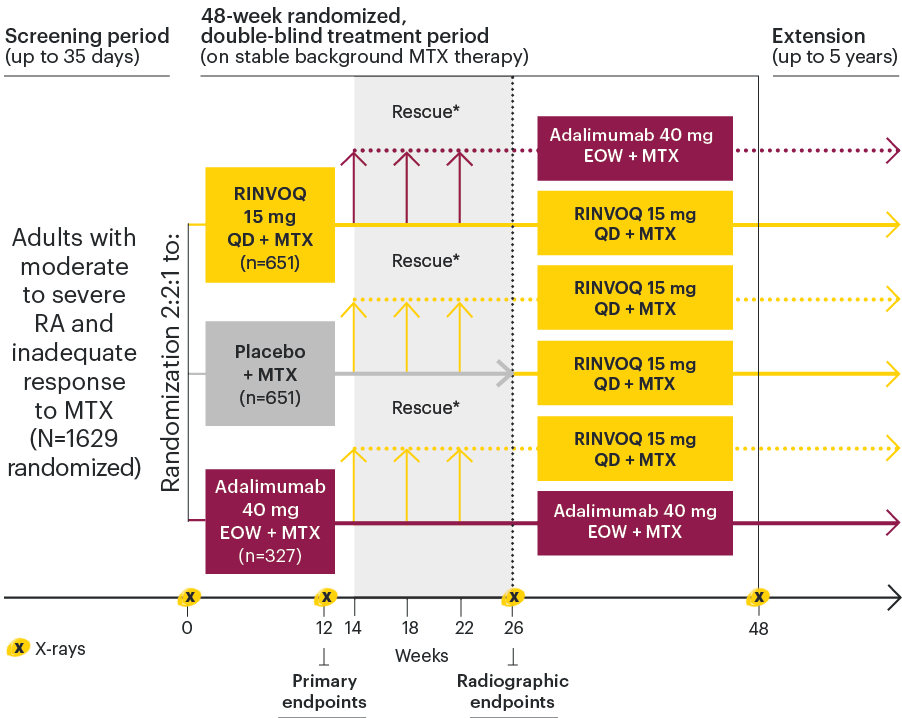
*Rescue criteria: At Weeks 14, 18, and 22, patients receiving adalimumab or placebo were switched to RINVOQ and patients receiving RINVOQ were switched to adalimumab if <20% improvement in tender joint count and swollen joint count vs baseline. At Week 26, all remaining placebo patients who were not rescued were switched to RINVOQ, and patients receiving RINVOQ or adalimumab were switched to adalimumab and RINVOQ, respectively, if CDAI >10.
Primary
RINVOQ 15 mg + MTX vs placebo + MTX at Week 12 for DAS28 (CRP) <2.6 (EMA) or ACR20 (FDA)
Safety
Adverse events, serious adverse events, adverse events of special interest (e.g., serious infections, opportunistic infections, MACEs, VTEs, malignancies)
- Patients ≥18 years of age were eligible to participate.
- Diagnosis of RA for ≥3 months fulfilling the 2010 ACR/EULAR classification for RA with active disease (≥6 swollen joints of 66, ≥6 tender joints of 68 examined, hsCRP ≥5 mg/L), and at least one of the following at screening: ≥3 erosions on x-rays of hands and feet, or ≥1 erosion and positivity for RF or ACCP.
- Patients must have had an inadequate response to MTX.
- Patients with prior exposure to at most 1 bDMARD (except adalimumab) were eligible (up to 20% of total study number of patients) if they had either limited exposure (<3 months) or had to discontinue the bDMARD due to intolerability.
- Patients with inadequate response to prior bDMARDs or prior exposure to a JAK inhibitor were excluded.
ACCP: anti-cyclic citrullinated protein; ACR: American College of Rheumatology; ACR20: improvement of at least 20% in the American College of Rheumatology core criteria; bDMARD: biological disease-modifying antirheumatic drug; CDAI: Clinical Disease Activity Index; DAS28 (CRP): disease activity score with 28-joint count (C-reactive protein); EMA: European Medicines Agency; EOW: every other week; EULAR: European League Against Rheumatism; FDA: Food & Drug Administration; hsCRP: high-sensitivity C-reactive protein; MACE: major adverse cardiovascular event; MTX: methotrexate; QD: once daily; RF: rheumatoid factor; VTE: venous thromboembolic event.

Significantly greater remission rates vs placebo + MTX and adalimumab + MTX (DAS28)
SELECT-COMPARE: Remission (DAS28 [CRP] <2.6) rates at Week 12 (NRI)1,2
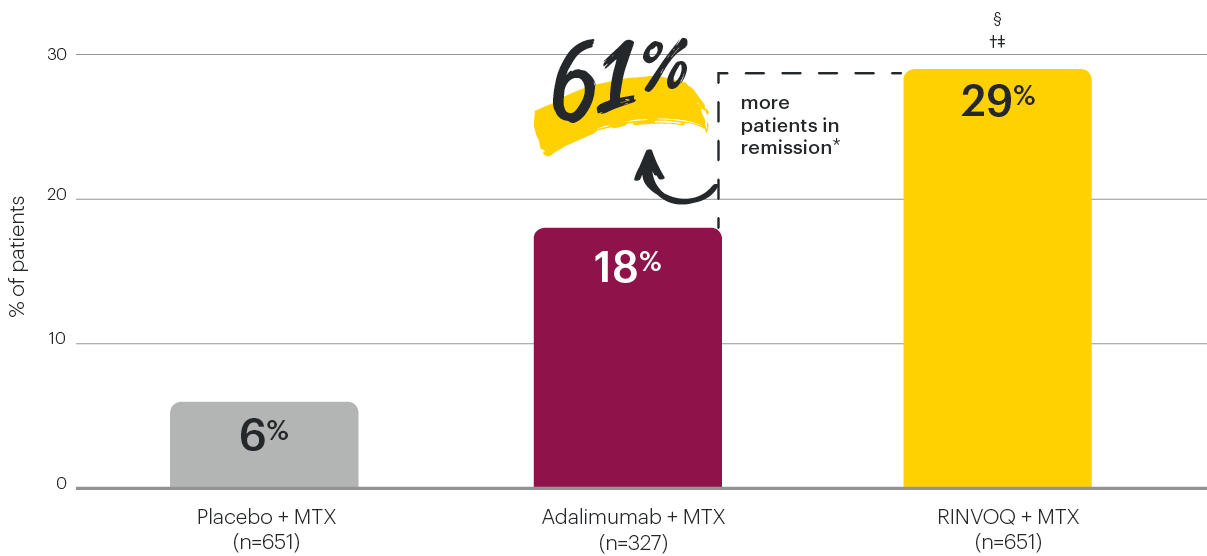


*61% is the relative difference between 29% (RINVOQ + MTX) and 18% (adalimumab + MTX) of patients who achieved remission (DAS28 [CRP] <2.6) at Week 12.
†P≤0.001 vs placebo + MTX
‡P≤0.001 vs adalimumab + MTX
§Indicates multiplicity-controlled comparison of RINVOQ + MTX vs placebo + MTX.
DAS28 (CRP) <2.6 for RINVOQ + MTX vs placebo + MTX at Week 12 was a primary endpoint controlled for multiplicity. DAS28 (CRP) <2.6 for RINVOQ + MTX vs adalimumab + MTX at Week 12 was a prespecified nonranked endpoint not controlled for multiplicity; nominal P-value is provided.
DAS28 (CRP): disease activity score with 28-joint count (C-reactive protein); MTX: methotrexate; NRI: nonresponder imputation.
Remission (DAS28 [CRP] <2.6) rates over time (NRI)
SELECT-COMPARE1-3


*P≤0.01 vs placebo + MTX
†P≤0.001 vs placebo + MTX
¶P≤0.01 vs adalimumab + MTX at Week 8
‡P≤0.01 vs adalimumab + MTX
§P≤0.001 vs adalimumab + MTX
IIIndicates multiplicity-controlled comparison of RINVOQ + MTX vs placebo + MTX.
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
††DAS28 (CRP) <2.6 for RINVOQ + MTX vs placebo + MTX at Week 12 was a primary multiplicity-controlled endpoint. All other data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using NRI (patients rescued at Weeks 14–22), and last observation carried forward (patients rescued at Week 26) for binary endpoints.
DAS28 (CRP): disease activity score with 28-joint count (C-reactive protein); MTX: methotrexate; NRI: nonresponder imputation.

RINVOQ + MTX remission rates across additional measures
SELECT-COMPARE: Remission rates at Week 12 (NRI)2
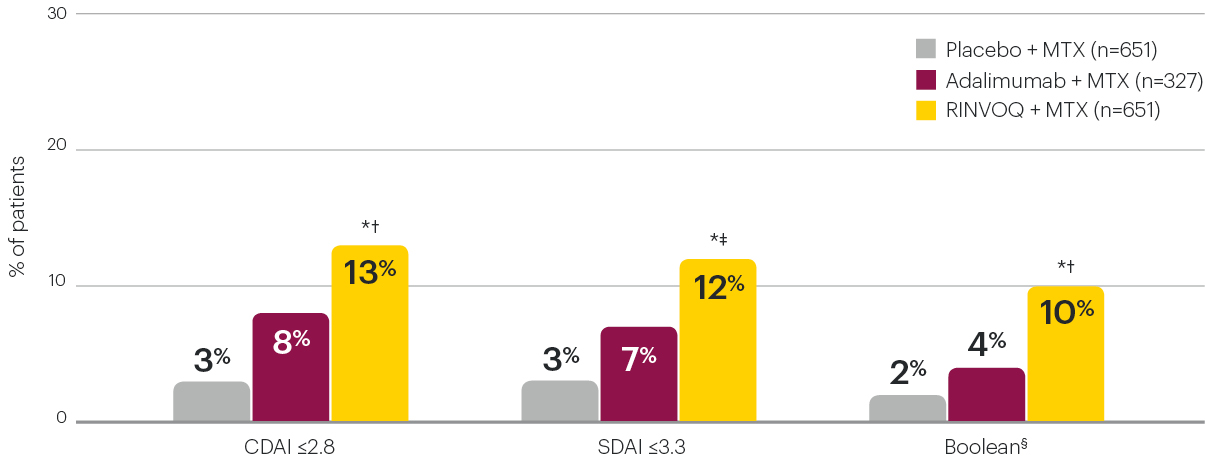
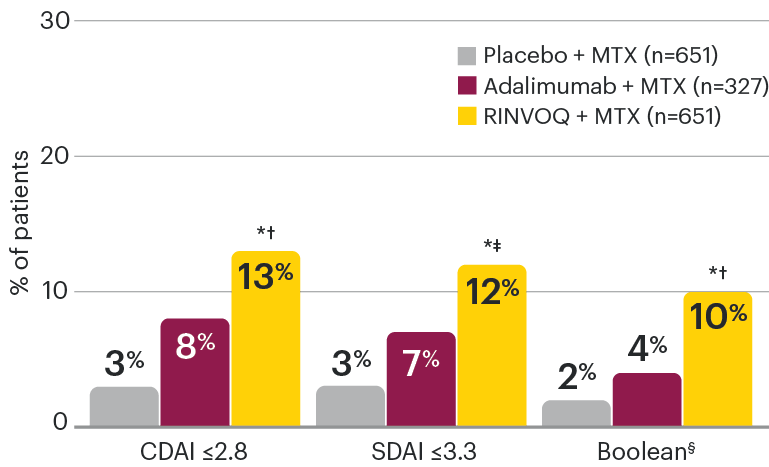
*P≤0.001 vs placebo + MTX
†P≤0.01 vs adalimumab + MTX
‡P≤0.05 vs adalimumab + MTX
§ACR/EULAR definition of remission: At any time point, a patient must satisfy all of the following: TJC ≤1, SJC ≤1, CRP ≤1 mg/dL, and PGA ≤1 (on a 0–10 scale).
Data shown are prespecified nonranked endpoints not controlled for multiplicity; nominal P-values are provided.
ACR: American College of Rheumatology; CDAI: Clinical Disease Activity Index; CRP: C-reactive protein; EULAR: European League Against Rheumatism; MTX: methotrexate; NRI: nonresponder imputation; PGA: Patient Global Assessment; SDAI: Simplified Disease Activity Index; SJC: swollen joint count; TJC: tender joint count.
Remission (CDAI ≤2.8) rates over time (NRI)
SELECT-COMPARE2,3


*P≤0.001 vs placebo + MTX
¶P≤0.01 vs adalimumab + MTX at Week 8
†P≤0.01 vs adalimumab + MTX
‡P≤0.001 vs adalimumab + MTX
§P≤0.05 vs adalimumab + MTX
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
All data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using NRI (patients rescued at Weeks 14–22), and last observation carried forward (patients rescued at Week 26) for binary endpoints.
CDAI: Clinical Disease Activity Index; MTX: methotrexate; NRI: nonresponder imputation.
Remission (SDAI ≤3.3) rates over time (NRI)
SELECT-COMPARE2,3


*P≤0.001 vs placebo + MTX
¶P≤0.05 vs adalimumab + MTX at Week 8
†P≤0.05 vs adalimumab + MTX
‡P≤0.01 vs adalimumab + MTX
§P≤0.001 vs adalimumab + MTX
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
All data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using NRI (patients rescued at Weeks 14–22), and last observation carried forward (patients rescued at Week 26) for binary endpoints.
MTX: methotrexate; NRI: nonresponder imputation; SDAI: Simplified Disease Activity Index.
Remission (Boolean#) rates over time (NRI)
SELECT-COMPARE2,3


*P≤0.001 vs placebo + MTX
¶P≤0.01 vs adalimumab + MTX at Week 4
†P≤0.01 vs adalimumab + MTX
‡P≤0.001 vs adalimumab + MTX
§P≤0.05 vs adalimumab + MTX
*Vertical line at Week 26 indicates the end of the placebo-controlled period.
All data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using NRI (patients rescued at Weeks 14–22), and last observation carried forward (patients rescued at Week 26) for binary endpoints.
#ACR/EULAR definition of remission: At any time point, a patient must satisfy all of the following: TJC ≤1, SJC ≤1, CRP ≤1mg/dL, and PGA ≤1 (on a 0–10 scale).
ACR: American College of Rheumatology; CRP: C-reactive protein; EULAR: European League Against Rheumatism; MTX: methotrexate; NRI: nonresponder imputation; PGA: Patient Global Assessment; SJC: swollen joint count; TJC: tender joint count.

RINVOQ + MTX was superior to adalimumab + MTX at Week 12 on:
SELECT-COMPARE2
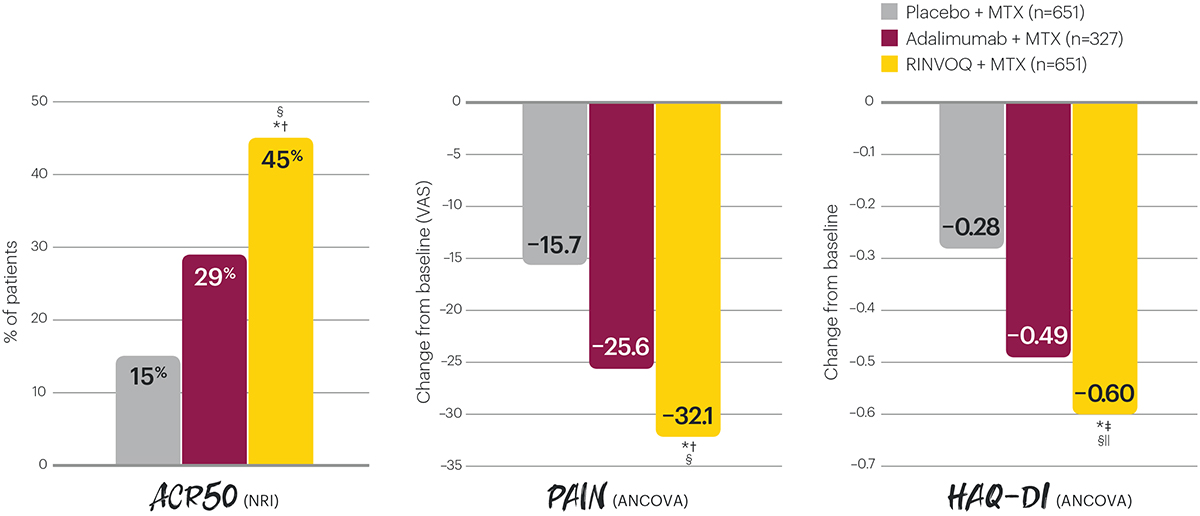
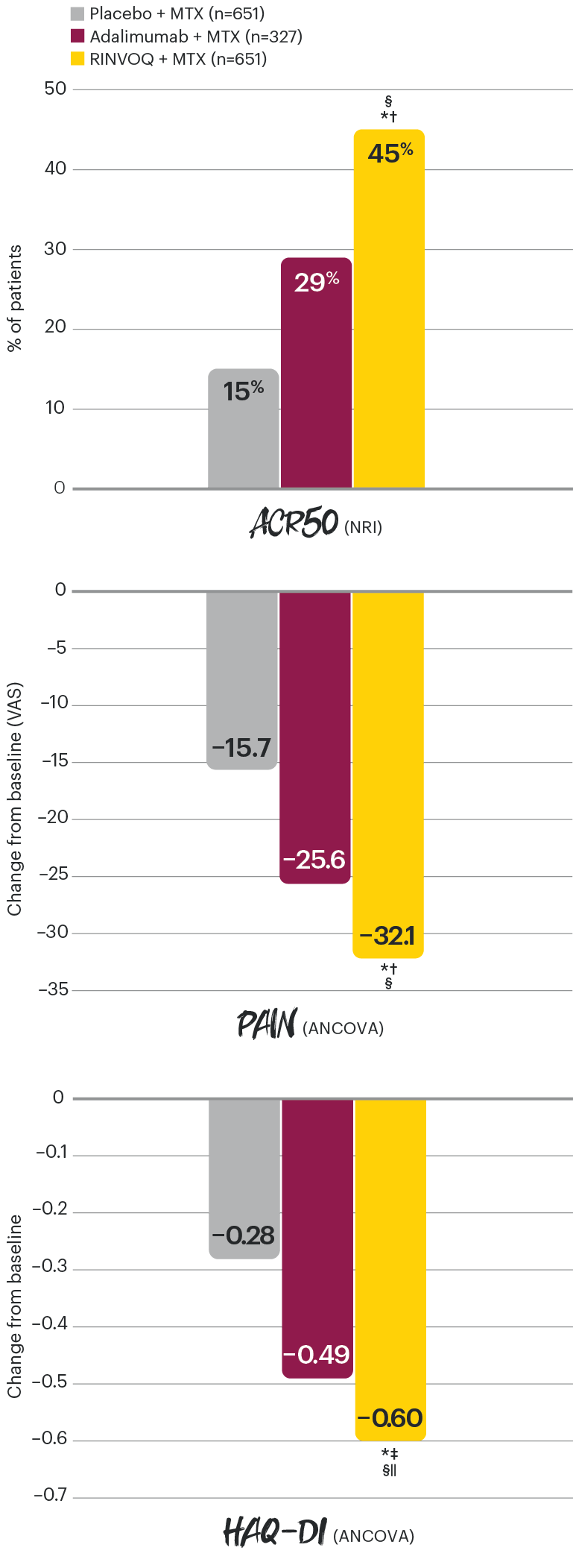
*P≤0.001 vs placebo + MTX
†P≤0.001 vs adalimumab + MTX
‡P≤0.01 vs adalimumab + MTX
§Indicates multiplicity-controlled superiority comparison of RINVOQ + MTX vs adalimumab + MTX.
IIIndicates multiplicity-controlled comparison of RINVOQ + MTX vs placebo + MTX.
Superiority for ACR50, Δ pain, and Δ HAQ-DI for RINVOQ + MTX vs adalimumab + MTX at Week 12 were ranked key secondary endpoints for FDA controlled for multiplicity. Δ HAQ-DI for RINVOQ + MTX vs placebo + MTX at Week 12 was a ranked key secondary endpoint for EMA controlled for multiplicity. All other data shown were prespecified nonranked endpoints not controlled for multiplicity; nominal P-values are provided.
ACR50: improvement of at least 50% in the American College of Rheumatology core criteria; ANCOVA: analysis of covariance; EMA: European Medicines Agency; FDA: Food and Drug Administration; HAQ-DI: Health Assesment Questionnaire Disabliity Index; MTX: methotrexate; NRI: nonresponder imputation; VAS: visual analogue scale.
ACR50 response rates over time (NRI)
SELECT-COMPARE1-3


*P≤0.001 vs placebo + MTX
†P≤0.05 vs adalimumab + MTX
‡P≤0.001 vs adalimumab + MTX
§P≤0.01 vs adalimumab + MTX
||Indicates multiplicity-controlled superiority comparison of RINVOQ + MTX vs adalimumab + MTX.
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
Superiority for ACR50 for RINVOQ + MTX vs adalimumab + MTX at Week 12 was an FDA ranked key secondary multiplicity-controlled endpoint. All other data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using NRI (patients rescued at Weeks 14–22), and last observation carried forward (patients rescued at Week 26) for binary endpoints.
ACR50: improvement of at least 50% in the American College of Rheumatology core criteria; MTX: methotrexate; NRI: nonresponder imputation.
Change in patient-reported pain (VAS) over time (ANCOVA)
SELECT-COMPARE2-4


*P≤0.001 vs placebo + MTX
†P≤0.001 vs adalimumab + MTX
‡P≤0.01 vs adalimumab + MTX
§P≤0.05 vs adalimumab + MTX
IIIndicates multiplicity-controlled superiority comparison of RINVOQ + MTX vs adalimumab + MTX.
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
Superiority for Δ pain for RINVOQ + MTX vs adalimumab + MTX at Week 12 was an FDA ranked key secondary multiplicity-controlled endpoint. All other data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using last observation carried forward for continuous endpoints.
ANCOVA: analysis of covariance; LOCF: last observation carried forward; MTX: methotrexate; VAS: visual analogue scale.
Change in HAQ-DI* over time (ANCOVA)
SELECT-COMPARE1-3


*Improvement in HAQ-DI is a reduction in score.
†P≤0.001 vs placebo + MTX
‡P≤0.05 vs adalimumab + MTX
§P≤0.01 vs adalimumab + MTX
IIP≤0.001 vs adalimumab + MTX
¶Indicates multiplicity-controlled superiority comparison of RINVOQ + MTX vs adalimumab + MTX.
#Indicates multiplicity-controlled comparison of RINVOQ + MTX vs placebo + MTX.
**Vertical line at Week 26 indicates the end of the placebo-controlled period.
Superiority for Δ HAQ-DI for RINVOQ + MTX vs adalimumab + MTX at Week 12 was an FDA ranked key secondary multiplicity-controlled endpoint. Δ HAQ-DI for RINVOQ + MTX vs placebo + MTX at Week 12 was an EMA ranked key secondary multiplicity-controlled endpoint. All other data shown were prespecified nonranked non–multiplicity-controlled endpoints; nominal P-values are provided.
Treatment groups are by initial randomization. Observations after rescue were handled using last observation carried forward for continuous endpoints.
ANCOVA: analysis of covariance; HAQ-DI: Health Assessment Questionnaire Disability Index; LOCF: last observation carried forward; LS: least squares; MTX: methotrexate.

RINVOQ: Joint protection over time
SELECT-COMPARE: Inhibition of structural joint damage progression at Week 26 (linear extrapolation)1,2

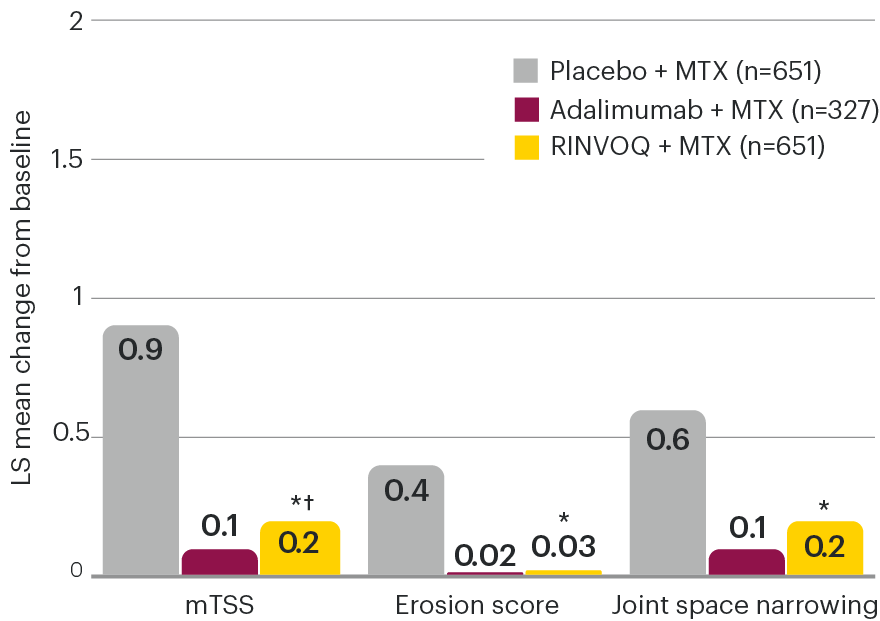
SELECT-COMPARE: Inhibition of structural joint damage progression at Week 48 (linear extrapolation)1,3


*P≤0.001 vs placebo + MTX
†Indicates multiplicity-controlled comparison of RINVOQ + MTX vs placebo + MTX.
Change in mTSS for RINVOQ + MTX vs placebo + MTX at Week 26 was a ranked secondary endpoint controlled for multiplicity. All other data shown for RINVOQ + MTX vs placebo + MTX were prespecified nonranked endpoints not controlled for multiplicity; nominal P-values are provided. No statistical comparisons were made between RINVOQ and adalimumab groups for radiographic endpoints.
Treatment groups are by initial randomization. For the placebo group, all data at Week 48 were imputed by linear extrapolation. X-ray data collected at treatment switching or at discontinuation of placebo (for patients who discontinued placebo) were used for extrapolation. Specifically, for placebo patients who switched to RINVOQ at Week 26, the Week 26 x-ray was used for extrapolation to impute the data at Week 48. For patients randomized to RINVOQ or adalimumab who were rescued, data at Week 48 were also imputed by linear extrapolation using x-ray data collected at treatment switching.1-3
LS: least squares; mTSS: modified total Sharp score; MTX: methotrexate; MTX-IR: inadequate response to MTX.

SELECT-COMPARE: Adverse events through 26 weeks of treatment2*
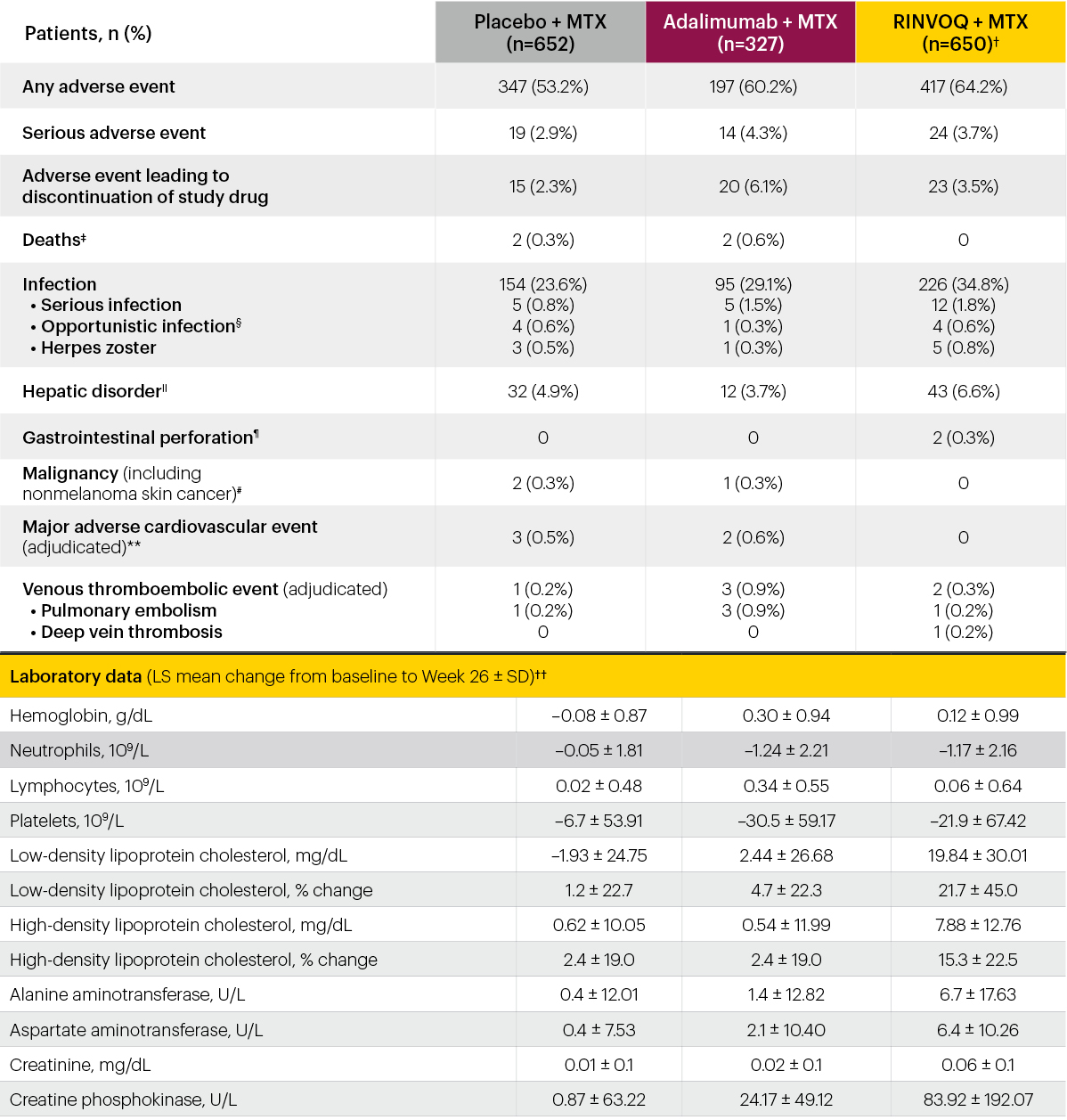
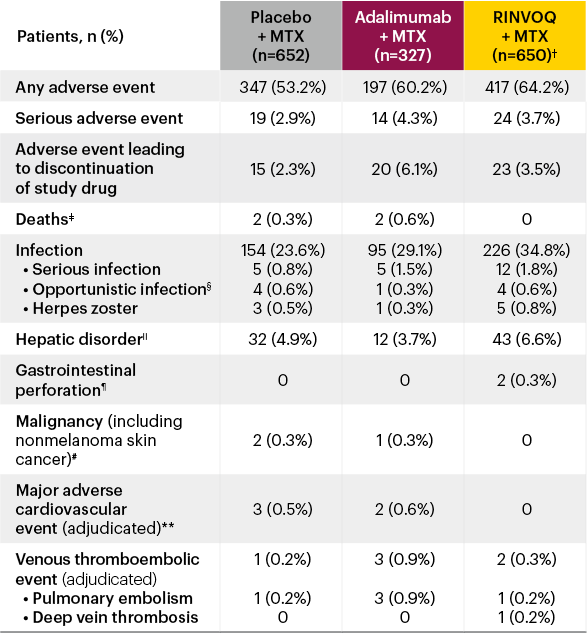




*Adverse events were collected and summarized up to Week 26 and censored as follows: For patients who remained on initially randomized treatment up to Week 26, all events up to Week 26 were included; for patients who met the rescue criteria at Week 14, 18, or 22, events that occurred starting the day of initiation of rescue treatment were excluded.
†One patient randomized to RINVOQ received only a placebo injection before discontinuing and is included in the placebo group for safety assessments.
‡Deaths: In the placebo + MTX group, there was 1 cardiovascular (CV) death and 1 death due to Pneumocystis jirovecii pneumonia. In the adalimumab + MTX group, there was 1 death due to craniocerebral injury and 1 CV death.
§Only 1 case of latent tuberculosis was reported (in the RINVOQ + MTX group).
IIHepatic disorders: Primarily liver function test elevation.
¶Gastrointestinal perforation (identified using GI perforation Standardized MedDRA Queries): not spontaneous perforations but 1 peritonitis and 1 anal abscess.
#Malignancies: In the placebo + MTX group, there was 1 cervical carcinoma and 1 basal cell carcinoma. In the adalimumab + MTX group, there was 1 basal cell carcinoma.
**Major adverse cardiovascular events (adjudicated): In the placebo + MTX group, there were 2 nonfatal myocardial infarctions and 1 CV death. In the adalimumab + MTX group, there was 1 nonfatal stroke and 1 CV death.
††Only patients who continued on initially randomized study drug are included in the analysis.
CPK: creatine phosphokinase; LS: least squares; MTX: methotrexate.
SELECT-COMPARE: Treatment-emergent adverse event summary through 48 weeks of treatment3*


SELECT-COMPARE: Percentage of patients with Grade 3/4 laboratory abnormalities through 48 weeks of treatment3#


*Investigator-reported treatment-emergent adverse events are summarized for events occurring while exposed to RINVOQ or adalimumab, based on the treatment received at the time of the event (“any RINVOQ,” “any adalimumab”). Exposure-adjusted event rates are reported (events/100 patient-years), and exposure-adjusted incidence rates are reported for deaths, major adverse cardiovascular events and venous thromboembolic events.
†In the RINVOQ + MTX group, there were 2 deaths due to undetermined/unknown cause, 1 due to cardiac failure, 1 sudden death, and 1 due to arteriosclerosis coronary artery. Among patients receiving adalimumab + MTX, there was 1 death due to left ventricular failure, 1 due to craniocerebral injury, 1 due to colon cancer, and 1 due to mixed connective tissue disease.
‡Hepatic disorders: majority were based on asymptomatic alanine aminotransferase/aspartate aminotransferase elevations.
§3 events of perforation (identified using GI perforation Standardized MedDRA) occurred in the RINVOQ + MTX group: 1 peritonitis with appendicitis in setting of a fallopian tube abscess, 1 anal abscess, and 1 anal fistula.
IIIn the RINVOQ + MTX group, there was 1 laryngeal cancer, 1 endometrial adenocarcinoma, 1 malignant melanoma, 1 adenocarcinoma gastric, and 1 adenocarcinoma of the colon reported. In the adalimumab + MTX group, there was 1 malignant melanoma, 1 colon cancer metastatic), and 1 lung neoplasm malignant reported.
¶Among patients receiving RINVOQ + MTX, there was 1 nonfatal stroke, 3 nonfatal Ml, and 1 CV death. In the adalimumab + MTX group, there was 1 nonfatal stroke and 1 CV death.
#Percentage of patients with Grade 3 or 4 laboratory abnormalities. Data is for patients with worsening in grade severity for laboratory parameters. Grading is based on OMERACT criteria, except for CPK and creatinine, where National Cancer Institute Common Toxicity Criteria are used.
ALT: alanine transaminase; AST: aspartate transaminase; CPK: creatine phosphokinase; CV: cardiovascular; EOW: every other week; Hb: hemoglobin; MI: myocardial infarction; MTX: methotrexate; OMERACT: Outcome Measures in Rheumatology; PY: patient-year; QD: once daily; ULN: upper limit of normal.

Safety Information1
RINVOQ is contraindicated in patients hypersensitive to the active substance or to any of the excipients, in patients with active tuberculosis (TB) or active serious infections, in patients with severe hepatic impairment, and during pregnancy.
Use in combination with other potent immunosuppressants is not recommended.
Serious and sometimes fatal infections have been reported in patients receiving upadacitinib. The most frequent serious infections reported included pneumonia and cellulitis. Cases of bacterial meningitis have been reported. Among opportunistic infections, TB, multidermatomal herpes zoster, oral/esophageal candidiasis, and cryptococcosis have been reported with upadacitinib. Prior to initiating upadacitinib, consider the risks and benefits of treatment in patients with chronic or recurrent infection or with a history of a serious or opportunistic infection, in patients who have been exposed to TB or have resided or traveled in areas of endemic TB or endemic mycoses, and in patients with underlying conditions that may predispose them to infection. Upadacitinib therapy should be interrupted if a patient develops a serious or opportunistic infection. As there is a higher incidence of infections in patients ≥65 years of age, caution should be used when treating this population.
Patients should be screened for TB before starting upadacitinib therapy. Anti-TB therapy should be considered prior to initiation of upadacitinib in patients with previously untreated latent TB or in patients with risk factors for TB infection.
Viral reactivation, including cases of herpes zoster, were reported in clinical studies. The risk of herpes zoster appears to be higher in Japanese patients treated with upadacitinib. Consider interruption of therapy if a patient develops herpes zoster until the episode resolves. Screening for viral hepatitis and monitoring for reactivation should be performed before starting and during therapy with upadacitinib.
The use of live, attenuated vaccines during or immediately prior to therapy is not recommended. It is recommended that patients be brought up to date with all immunizations, including prophylactic zoster vaccinations, prior to initiating upadacitinib, in agreement with current immunization guidelines.
The risk of malignancies, including lymphoma is increased in patients with rheumatoid arthritis (RA). Immunomodulatory medicinal products may increase the risk of malignancies, including lymphoma. The clinical data are currently limited and long-term studies are ongoing. Malignancies, including nonmelanoma skin cancer (NMSC), have been reported in patients treated with upadacitinib. Consider the risks and benefits of upadacitinib treatment prior to initiating therapy in patients with a known malignancy other than a successfully treated NMSC or when considering continuing upadacitinib therapy in patients who develop a malignancy. Periodic skin examination is recommended for patients who are at increased risk for skin cancer.
Absolute neutrophil count <1000 cells/mm3, absolute lymphocyte count <500 cells/mm3, or hemoglobin levels <8 g/dL were reported in ≤1% of patients in clinical trials. Treatment should not be initiated, or should be temporarily interrupted, in patients with these hematological abnormalities observed during routine patient management.
RA patients have an increased risk for cardiovascular disorders. Patients treated with upadacitinib should have risk factors (e.g., hypertension, hyperlipidemia) managed as part of usual standard of care.
Upadacitinib treatment was associated with increases in lipid parameters, including total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol. The effect of these lipid parameter elevations on cardiovascular morbidity and mortality has not been determined.
Treatment with upadacitinib was associated with an increased incidence of liver enzyme elevation compared to placebo. If increases in ALT or AST are observed during routine patient management and drug-induced liver injury is suspected, upadacitinib therapy should be interrupted until this diagnosis is excluded.
Events of deep vein thrombosis (DVT) and pulmonary embolism (PE) have been reported in patients receiving JAK inhibitors, including upadacitinib. Upadacitinib should be used with caution in patients at high risk for DVT/PE. Risk factors that should be considered in determining the patient’s risk for DVT/PE include older age, obesity, a medical history of DVT/PE, patients undergoing major surgery, and prolonged immobilization. If clinical features of DVT/PE occur, upadacitinib treatment should be discontinued and patients should be evaluated promptly, followed by appropriate treatment.
The most commonly reported adverse drug reactions (ADRs) were upper respiratory tract infections, bronchitis, nausea, blood creatine phosphokinase (CPK) increased, and cough. The most common serious adverse reactions were serious infections.
Please see the RINVOQ Summary of Product Characteristics for complete Prescribing Information.


I want to receive more information via a product specialist.
I have a question for Medical Information.
References
- RINVOQ [Summary of Product Characteristics]. AbbVie Deutschland GmbH & Co. KG; May 2021.
- Fleischmann R, Pangan AL, Song IH, et al. Upadacitinib versus placebo or adalimumab in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a phase III, double-blind, randomized controlled trial. Arthritis Rheumatol. 2019;71(11):1788-1800. doi:10.1002/art.41032
- Fleischmann RM, Genovese MC, Enejosa JV, et al. Safety and effectiveness of upadacitinib or adalimumab plus methotrexate in patients with rheumatoid arthritis over 48 weeks with switch to alternate therapy in patients with insufficient response. Ann Rheum Dis. 2019;78(11):1454-1462. doi:10.1136/annrheumdis-2019-215764
- Fleischmann R, Enejosa JV, Song IH, et al. Safety and effectiveness of upadacitinib or adalimumab in patients with rheumatoid arthritis: results at 48 weeks from the SELECT-COMPARE study. Abstract presented at: European Congress of Rheumatology; June 12–15, 2019; Madrid, Spain.